First-in-human phase I study of EGF816, a thirdgeneration, mutant-selective EGFR tyrosine kinase inhibitor, in advanced non-small cell lung cancer (NSCLC) harboring T790M.
Sub-category:
Lung Cancer—Non-Small Cell Metastatic
Category:
Lung Cancer—Non-Small Cell Metastatic
Meeting:
2015 ASCO Annual Meeting
Abstract No:
8013
Poster Board Number:
Board #335
Citation:
J Clin Oncol 33:5s, 2015 (suppl; abstr 8013)
Author(s): Daniel Shao-Weng Tan, Takashi Seto, Natasha B. Leighl, Gregory J. Riely, Lecia V. Sequist, Enriqueta Felip, Juergen Wolf, James Chih-Hsin Yang, Igor Matushansky, Xiaolu Yu, Shu-Fang Hsu Schmitz, Xiaoming Cui, Dong-Wan Kim; National Cancer Centre Singapore, Singapore, Singapore; National Kyushu Cancer Center, Fukuoka, Japan; Princess Margaret Hospital, Toronto, ON, Canada; Memorial Sloan Kettering Cancer Center, New York, NY; Massachusetts General Hospital, Boston, MA; Vall d'Hebron University Hospital, Barcelona, Spain; Department I of Internal Medicine and Center of Integrated Oncology Cologne Bonn, University Hospital Cologne, Cologne, Germany; National Taiwan University Hospital and National Taiwan University, Taipei, Taiwan; Novartis Pharmaceuticals Corporation, East Hanover, NJ; China Novartis Institutes for BioMedical Research, Shanghai, China; Novartis Pharma AG, Basel, Switzerland; Seoul National University Hospital, Seoul, South Korea
Abstract Disclosures
Abstract:
Background: The emergence of T790M resistance mutations (mt) occurs in up to 50% of patients (pt) with NSCLC harboring a sensitizing EGFR mt treated with erlotinib or gefitinib. EGF816 is a covalent, irreversible, EGFR TKI that has nanomolar inhibitory potency against activating mt (L858R, ex19del) and T790M mt, with up to 60-fold selectivity over wild type (wt) EGFR in vitro. Methods:This multicenter, dose escalation study to determine the safety, tolerability and antitumor activity of EGF816, enrolled NSCLC pts with locally or centrally confirmed T790M status. Oral EGF816 was administered on a continuous 28-day schedule. Dose escalation started from 75 mg QD and was guided by an adaptive Bayesian logistic regression model to determine the maximum tolerated dose. Paired tumor biopsies were performed to evaluate pharmacodynamics. NCT02108964. Results: As of 26 Jan 2015, 57 pts have been treated (51 capsules, CAP; 6 tablets, TAB) across 6 cohorts (75, 150, 225, 300, and 350 mg for CAP; 225 mg for TAB). At the 4 Dec 2014 cutoff, 40 pts were evaluable for safety, median age 58.5y (range 34–76), 48% male and 80% East Asian. 2/6 pts experienced DLT at 350 mg (rash, n = 2; acute renal injury, n = 1). The most common adverse events (AE) regardless of study drug relationship were diarrhea (25%), stomatitis (22.5%), rash (17.5%) and pruritus (15%). The most common Grade 3/4 drug-related AE was rash (5%). RECIST responses and reduced pEGFR were observed at all dose levels. Amongst 22 evaluable pts, including 1 with de novoT790M mt, ORR (including unconfirmed responses) and disease control rate was 54.5% and 86.4% respectively. Only 1 pt experienced progressive disease at first evaluation – repeat testing revealed the tumor to be EGFR wt. PK shows rapid absorption with a median Tmax of 3h and dose-proportional increases in Cmax and AUC(0-tau) observed after single and multiple dosing. Conclusions: EGF816 is well tolerated with a manageable safety profile and antitumor activity against T790M mt NSCLC across all dose levels examined. Further study is ongoing to establish the optimal dose range to maximize therapeutic potential and facilitate future combinations. Clinical trial information:NCT02108964
TIGER 1: A randomized, open-label, phase 2/3 study of rociletinib (CO-1686) or erlotinib as first-line treatment for EGFR-mutant non-small cell lung cancer (NSCLC).
Sub-category:
Lung Cancer—Non-Small Cell Metastatic
Category:
Lung Cancer—Non-Small Cell Metastatic
Meeting:
2015 ASCO Annual Meeting
Abstract No:
TPS8108
Poster Board Number:
Board #430a
Citation:
J Clin Oncol 33:5s, 2015 (suppl; abstr TPS8108)
Author(s): D. Ross Camidge, Juergen Wolf, Jason B. Litten, Linda A Higashi, Jeffrey D. Isaacson, Tony Mok; University of Colorado Cancer Center, Aurora, CO; Department I of Internal Medicine and Center of Integrated Oncology Cologne Bonn, University Hospital Cologne, Cologne, Germany; Clovis Onccology, San Francisco, CA; Clovis Oncology, Englewood, NJ; Clovis Onc, Boulder, CO; Chinese University of Hong Kong, Shatin, Hong Kong
Abstract Disclosures
Abstract:
Background: Activating EGFR mutations including exon 21 L858R and exon 19 deletions (del19) are key drivers of NSCLC in 10%–15% of patients (pts) of European and 30%–35% of Asian descent.1Acquired resistance (AR) to first-generation EGFR tyrosine kinase inhibitors (TKIs) such as erlotinib is driven by additional EGFR mutations, with exon 20 T790M accounting for 60%–70% of cases.2Rociletinib (CO-1686) was designed to inhibit T790M as well as L858R and del19 while sparing wild-type EGFR and has demonstrated response rates up to 67% and is well tolerated in pts with AR to EGFR-TKIs during dose-finding studies.3TIGER 1 will evaluate whether rociletinib can improve progression-free survival (PFS) in the first-line setting. Novel exploratory endpoints include tumor kinetics, treatment post-progression, circulating tumor DNA, and blood-based biomarkers. Methods: Pts with histologically or cytologically confirmed metastatic or unresectable locally advanced recurrent NSCLC (no prior EGFR TKI therapy and no CNS disease), with documentation of ≥ 1 activating EGFR mutation (excluding exon 20 insertions) will be enrolled in this phase 2, open-label study (NCT02186301). Pts will be randomized 1:1 to rociletinib (625 mg) twice daily or erlotinib (150 mg) once daily until disease progression according to RECIST 1.1. Pts will be stratified by sensitizing EGFR mutation (T790M, del19, L858R, or other) and race (Asian vs non-Asian). The primary endpoint is PFS; secondary endpoints include efficacy as determined by objective response rate, duration of response, disease control rate and overall survival, and PFS in pts with baseline T790M mutations detected using allele-specific PCR. PFS and OS will be summarized with Kaplan-Meier plots. The stratified log-rank and hazard ratio will compare PFS distributions for rociletinib- vs erlotinib-treated pts. Safety will be assessed via standard adverse event reporting. Planned enrollment is for phase 2 is 200 pts up to 1000 for phase 3. Enrollment is underway with multiple patients in screening.
Herbst R et al. N Engl J Med. 2008
Yu H et al. Clin Cancer Res. 2013
Sequist LV J Clin Oncol. 2014
Clinical trial information: NCT02186301
|
 肺腺癌术后Her2扩增要不要加免疫?
麻烦问下,父亲刚做了派特CT,目前考虑都是炎性,没有转移,术后化疗四次了,her2扩
肺腺癌术后Her2扩增要不要加免疫?
麻烦问下,父亲刚做了派特CT,目前考虑都是炎性,没有转移,术后化疗四次了,her2扩
 盲试靶向药 29个月,治疗分享
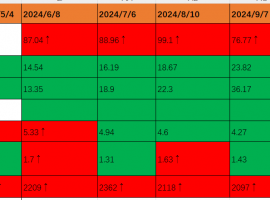
时间:2025/1/27 盲试靶向药第29个月。
本月治疗方案:7080(14mg)。2024年11月底
盲试靶向药 29个月,治疗分享
时间:2025/1/27 盲试靶向药第29个月。
本月治疗方案:7080(14mg)。2024年11月底
![[咨询交流]化免半年后出现脚红肿的症状,是否需要使用激素?](data/attachment/block/4f/4f97475509b0f241b92496b4766a94d3.jpg) [咨询交流]化免半年后出现脚红肿的
肺腺癌Ⅳa期,方案是k药+培美曲塞进行了约半年,肿瘤缩小目前无进展,但这周出现脚红
[咨询交流]化免半年后出现脚红肿的
肺腺癌Ⅳa期,方案是k药+培美曲塞进行了约半年,肿瘤缩小目前无进展,但这周出现脚红
 食管癌:我会平等地创飞每一个忽视我
众所周知,中国人常“民以食为天”,爱吃应该算是每一个中国
食管癌:我会平等地创飞每一个忽视我
众所周知,中国人常“民以食为天”,爱吃应该算是每一个中国
 肺癌晚期三代靶向药耐药后,我为自己
讲述者:薰衣草整理者:pear
2022年6月我确诊肺癌晚期,虽有EGFR突变,但我却对靶向药
肺癌晚期三代靶向药耐药后,我为自己
讲述者:薰衣草整理者:pear
2022年6月我确诊肺癌晚期,虽有EGFR突变,但我却对靶向药





 eltarasin, a small molecule inhibitor of KRAS-PDEδ interaction, provides a unique opportunity to target KRAS mutant NSCLC.
eltarasin, a small molecule inhibitor of KRAS-PDEδ interaction, provides a unique opportunity to target KRAS mutant NSCLC. 显身卡
显身卡

![[咨询交流]化免半年后出现脚红肿的症状,是否需要使用激素?](data/attachment/block/db/db81396fd2c4e4b663841732d9c28cd5.jpg)