Exelixis, Inc. reported expanded Phase 2 study data with respect to cabozantinib (XL184) use in advanced ovarian cancer patients at the 2011 American Society of Clinical Oncology (ASCO) Annual Meeting . The overall solid tumor Phase 2 safety and tolerability data refers to six deaths, including two ovarian cancer patients.
On May 19, 2011, we reported promising cabozantinib phase 2 solid tumor (including ovarian) data, which was presented at an ASCO press briefing held in advance of the 2011 ASCO Annual Meeting. As noted in our May 19 article, cabozantinib demonstrated excellent activity against several solid tumors, including ovarian cancer. In addition, we reported that cabozantinib showed promising activity in ovarian cancer patients independent of prior response to platinum drug-based therapies.
Ronald J. Buckanovich, M.D., Ph.D., Assistant Professor, Departments of Internal Medicine & Obstetrics and Gynecology, University of Michigan, presented the expanded cabozantinib Phase 2 data relating to use of the drug in advanced ovarian cancer patients, on June 4 at the 2011 ASCO Annual Meeting.
Ovarian Cancer Patient Population & Overall Response Rate
(Image Source: Exelixis, Inc.)
The cabozantinib trial is an ongoing phase 2 adaptive randomized discontinuation trial. As of the February 11, 2011 cut-off date, accrual in the cabozantinib study cohort was complete at 70 patients.
The 70 patients enrolled in the ovarian cancer cohort received oral cabozantinib (100 mg) daily over a 12 week “Lead-in Stage.” These patients had a minimum follow-up of at least 12 weeks and were thus evaluable for safety and the primary efficacy endpoint of response per RECIST (Response Evaluation Criteria in Solid Tumors).
Patient tumor response was assessed every 6 weeks. Receipt of cabozantinib treatment beyond the 12 week open label Lead-in Stage was based upon patient response: (1) patients with a partial response (PR) or complete response (CR) continued taking cabozantinib, (2) patients with stable disease (SD) were randomized to the cabozantinib treatment arm or the placebo treatment arm (collectively referred to as the “Blinded Randomized Stage”), and (iii) patients with progressive disease (PD) discontinued study treatment. The study primary endpoint was overall response rate (ORR) per RECIST in the Lead-in Stage, and progression free survival (PFS) in the Blinded Randomized Stage. Accrual in any cohort could be halted for high ORR or PD.
Approximately half of the 70 patients enrolled in the cohort were considered platinum drug-refractory/-resistant (49%), defined as a platinum drug-free interval of 6 months or less, and the remainder of patients (51%) had platinum-sensitive disease based on a platinum-free interval greater than 6 months.
The baseline patient tumor histologic characteristics are as follows: serous ovarian cancer (79%), clear cell ovarian cancer (4%), endometrioid ovarian cancer (6%), and other forms of ovarian cancer (11%)
More than half the patients (57%) received 2 or more prior lines of platinum therapy prior to trial enrollment. Some patients also had additional prior lines of therapy with agents such as pegylated liposomal doxorubicin (brand name: Doxil®) or topotecan (brand name: Hycamtin®) (32%), gemcitabine (brand name: Gemzar®) (29%), and VEGF (vascular endothelial growth factor) pathway inhibitors (10%).
Evidence of objective tumor regression was observed in 73% of patients with at least 1 post-baseline medical imaging scan. The best overall response rate per RECIST criteria was 24% (16 PRs and 1 CR). The overall Week-12 disease control rate (DRC = CR + PR + SD) was 53%. The Week-12 DCRs in the platinum drug-refractory, -resistant, and -sensitive groups were 36%, 39%, and 67%, respectively.
Based on an observed high rate of clinical activity, randomization was halted, and randomized patients were unblinded. At this point, the unblinded randomized patients that were treated with placebo were allowed to “cross-over” to treatment with cabozantinib. Disease stabilization was experienced by some ovarian cancer patients who had progressive disease prior to treatment cross-over.
“These latest results in metastatic ovarian cancer demonstrate the potential broad utility of cabozantinib beyond bone-predominant types of cancers such as castration-resistant prostate cancer. The high rates of durable response with our dual inhibitor of MET and VEGFR2 compare favorably to those of other single-agent targeted therapies and cytotoxic agents in development,” said Michael M. Morrissey, Ph.D., president and chief executive officer of Exelixis. “These results underscore the potential of cabozantinib in metastatic ovarian cancer, and we are in discussions with leading cooperative groups to plan further evaluation of cabozantinib in randomized trials for this indication.”
Activity in Platinum Drug-Sensitive, -Refractory, and -Resistant Disease
Ignace Vergote, M.D., Ph.D., senior author of the cabozantinib (XL184) ASCO presentation & Chairman, Leuven Cancer Institute, University of Leuven, European Union
(Image Source: Exelixis, Inc.)
Two of 11 patients (18%) with platinum refractory disease, defined as a platinum-free interval of <1 month, achieved a confirmed response (1 CR and 1 PR).
In the subset of patients with platinum-resistant disease, defined as a platinum-free interval of 1-6 months, 5 of 23 (22%) achieved a PR.
Ten of 36 patients (28%) with platinum sensitive disease achieved a PR.
A total of 37 patients experienced reductions in the ovarian cancer tumor marker CA-125 (cancer antigen-125), including 8 with decreases greater than 50%. There is no consistent concordance between CA-125 changes and tumor regression. The median duration of response has not yet been reached with 36 weeks of median follow-up.
“The continued activity of cabozantinib in a larger population of ovarian cancer patients is very encouraging, especially with respect to the clinical benefit observed in both platinum-sensitive and platinum-resistant/refractory disease. This activity profile has not been observed with other single-agent TKIs [tyrosine kinase inhibitors], and cabozantinib has the potential to be an important new treatment for ovarian cancer,” said Ignace Vergote, M.D., Ph.D., senior author of the presentation and Chairman of the Leuven Cancer Institute at the University of Leuven, European Union. “The high rate of disease control in platinum-resistant and platinum-refractory disease suggests that cabozantinib may help to address the substantial unmet medical need faced by patients who have sub-optimal responses to platinum-based therapies. I believe that further evaluation will help to define the potential role of cabozantinib in the treatment of ovarian cancer.”
General Safety & Tolerability Data
Safety data are available for the 70 patients in the Lead-In phase of the cabozantinib study. The most common CTCAE (Common Terminology Criteria for Adverse Events) grade 3 or 4 adverse events (AEs), regardless of causality, were diarrhea (10%), fatigue (9%), palmar-plantar erythrodysesthesia syndrome (also referred as “hand-foot syndrome”)(7%), vomiting (4%), abdominal pain (3%), hypomagnesemia (3%), and nausea, constipation, rash, increased transaminase, and hypertension (each 1%). At least one dose reduction was reported in 37% of patients. Less frequent important medical events, regardless of causality, were hemorrhage (11% all CTCAE grades, 0% CTCAE grade 3 or 4), venous thrombosis (6% all CTCAE grades, 4% CTCAE grade 3 or 4), and gastrointestinal perforation (6% all CTCAE grades, 0% CTCAE grade 3 or 4).
To access the cabozantinib clinical study data information, please visit www.exelixis.com/sites/default/f ... 1-XL184-Ovarian.pdf
Six Deaths Reported (Including Two Ovarian Cancer Patients)
If you examine the Exelixis press release dated June 4 (entitled, Exelixis’ Cabozantinib Demonstrates Encouraging Clinical Activity in Patients with Metastatic Ovarian Cancer – Disease control rate of 53% at week 12, response rate of 24%), which addresses data for cabozantinib use in advanced ovarian cancer patients, pay particular attention to the wording under the heading entitled, “Safety and Tolerability.” Within the wording set forth under that heading, you will find the following statement: “Two cabozantinib-related grade 5 AEs [adverse events], one enterocutaneous fistula and one intestinal perforation, were reported after the Lead-In phase.” Pursuant to the CTCAE guidelines, a “grade 5 adverse event” is defined as “death related to AE [adverse event].”
We should also note that the two ovarian cancer deaths were summarized briefly in the ASCO presentation regarding cabozantinib use in advanced ovarian cancer.
The reporting of all six deaths is set forth in the Exelixis press release, dated June 5, 2011 (entitled, Exelixis’ Cabozantinib Demonstrates Broad Clinical Activity in Multiple Tumor Types), in similar fashion. Within this release, the sentence provided under the heading “Safety and Tolerability” states: “There were 6 (1%) cabozantinib-related grade 5 [adverse] events, all of which were reported after the Lead-In phase of the trial: respiratory compromise (breast cancer), hemorrhage (NSCLC [non-small cell lung cancer]), enterocutaneous perforation (ovarian cancer), intestinal perforation (ovarian cancer), gastrointestinal hemorrhage (pancreatic cancer), and death (CRPC [castrate resistant prostate cancer]).”
Exelixis Chief Executive Michael Morrissey said the safety statistics are consistent with targeted cancer therapies like cabozantinib that block a pathway used by tumor cells to secure blood vessels.
Cowen & Co analyst Eric Schmidt said the rate of cabozantinib treatment-related deaths — 1 percent — was “no different from what we have seen for every other Phase 1 and 2 trials here at ASCO.”
“While drug safety is of less concern in cancer indications than in others, the apparent morbidities associated with cabo[zantinib] use will confound interpretation of clinical benefit in a trial designed to show anything less than overall survival,” Canaccord analyst George Farmer said in a research note.
In a note to investors, Piper Jaffray analyst Edward Tenthoff said: ”The company is exploring lower doses, but the concern is that cabo[zantinib] will not retain the impressive efficacy seen to date.”
Mr. Morrissey said Exelixis plans to move forward with the current daily 100 mg dose of the drug.
Dr. Nicholas J. Vogelzang (Director, Comprehensive Cancer Centers of Nevada) Discusses Mortalities in the Cabozantinib (XL184) Trial
XL184起始服用剂量:100mg |
 乙状结肠癌肝肺转移
乙状结肠癌肝肺转移,现已经做了第一阶段的治疗,介入奥沙,加口服卡培滨,复方斑蝥胶
乙状结肠癌肝肺转移
乙状结肠癌肝肺转移,现已经做了第一阶段的治疗,介入奥沙,加口服卡培滨,复方斑蝥胶
 重启化疗后疼痛一直加重,是化疗无效
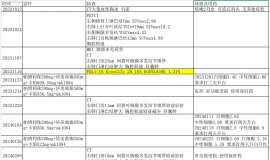
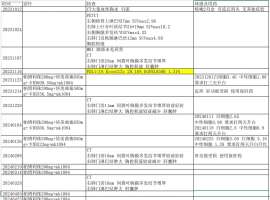
治疗经过如下:
Kras G12c 20.16%附带一个1.31%丰度的egfr21 PDL1阴性
靶向药的课题
重启化疗后疼痛一直加重,是化疗无效
治疗经过如下:
Kras G12c 20.16%附带一个1.31%丰度的egfr21 PDL1阴性
靶向药的课题
 依沃西用药后,该怎么办?
依沃西用药后,该怎么办?
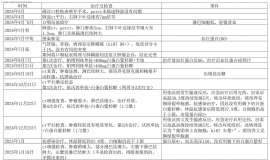
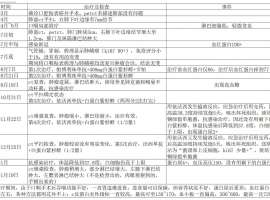
我爸爸于2024年7月确诊肺鳞癌,整个治疗过程如附件里表格
依沃西用药后,该怎么办?
依沃西用药后,该怎么办?
我爸爸于2024年7月确诊肺鳞癌,整个治疗过程如附件里表格
 妈妈与脑膜转奋战4年多,如今也成功
作者:李妮妮
2020年12月1号,妈妈在确诊晚期肺癌4年零10月,经历了化疗、一代靶向易
妈妈与脑膜转奋战4年多,如今也成功
作者:李妮妮
2020年12月1号,妈妈在确诊晚期肺癌4年零10月,经历了化疗、一代靶向易
 初诊必看:肿瘤患者诊断时最关心的10
作者:赵行
治不治
有人说,给父母看病治病天经地义,这是个值得讨论的话题吗?
我
初诊必看:肿瘤患者诊断时最关心的10
作者:赵行
治不治
有人说,给父母看病治病天经地义,这是个值得讨论的话题吗?
我





 显身卡
显身卡