| |
| |
| |
| |
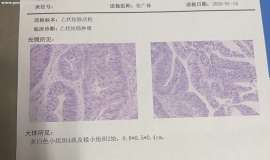
 乙状结肠癌肝肺转移
乙状结肠癌肝肺转移,现已经做了第一阶段的治疗,介入奥沙,加口服卡培滨,复方斑蝥胶
乙状结肠癌肝肺转移
乙状结肠癌肝肺转移,现已经做了第一阶段的治疗,介入奥沙,加口服卡培滨,复方斑蝥胶
 重启化疗后疼痛一直加重,是化疗无效
治疗经过如下:
Kras G12c 20.16%附带一个1.31%丰度的egfr21 PDL1阴性
靶向药的课题
重启化疗后疼痛一直加重,是化疗无效
治疗经过如下:
Kras G12c 20.16%附带一个1.31%丰度的egfr21 PDL1阴性
靶向药的课题
 依沃西用药后,该怎么办?
依沃西用药后,该怎么办?
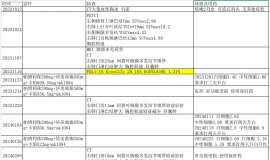
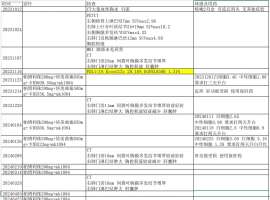
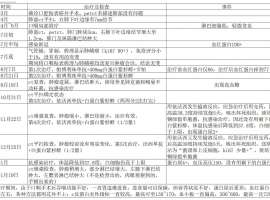
我爸爸于2024年7月确诊肺鳞癌,整个治疗过程如附件里表格
依沃西用药后,该怎么办?
依沃西用药后,该怎么办?
我爸爸于2024年7月确诊肺鳞癌,整个治疗过程如附件里表格
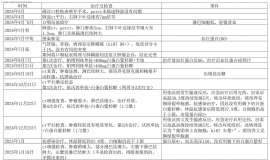
 妈妈与脑膜转奋战4年多,如今也成功
作者:李妮妮
2020年12月1号,妈妈在确诊晚期肺癌4年零10月,经历了化疗、一代靶向易
妈妈与脑膜转奋战4年多,如今也成功
作者:李妮妮
2020年12月1号,妈妈在确诊晚期肺癌4年零10月,经历了化疗、一代靶向易
 初诊必看:肿瘤患者诊断时最关心的10
作者:赵行
治不治
有人说,给父母看病治病天经地义,这是个值得讨论的话题吗?
我
初诊必看:肿瘤患者诊断时最关心的10
作者:赵行
治不治
有人说,给父母看病治病天经地义,这是个值得讨论的话题吗?
我





 显身卡
显身卡